





Physiology IDC Dive Theory
- Tracy Gunn
- Jun 8, 2023
- 27 min read
Updated: Jan 24, 2024

Struggling with Physiology during your Instructor Development. The following information will discuss basic diving physiology and attend to many of the questions that you will find in your IE. There are exams built-in along the way to help test your knowledge.
THE BODY SYSTEM AND THE EFFECTS OF GASES
The purpose of the respiratory and circulatory systems is to supply tissues with Oxygen and to remove Carbon Dioxide: the two gases most important to your metabolic processes.

The circulatory system transports oxygen, fuels, and materials from the respiratory and digestive systems to your body tissues.
It carries waste, CO2 and other wastes from your tissues for elimination.
The gas exchange between the tissues and the blood occurs in capillaries throughout the body.
The respiratory system brings oxygen to the body and carries waste carbon dioxide out. Gas exchange between the respiratory and circulatory systems occurs between the alveoli and the pulmonary capillaries. It is here that the blood releases carbon dioxide and picks up oxygen.
BLOOD

Plasma:
Carries nutrients, chemicals, and dissolved gases, including some waste carbon dioxide and nitrogen. Plasma accounts for half the weight of blood.
Red blood cells (erythrocytes):
Carries most of the oxygen required via haemoglobin, a protein that bonds and unbonds with oxygen. Without haemoglobin, the blood would have to circulate the plasma 15 to 20 times faster to supply a resting body with sufficient oxygen. Red blood cells make up about 45% of the blood.
Haemoglobin
Carries and releases oxygen efficiently because variations in oxygen partial pressure influence its capacity to remain bonded with oxygen. 5% of the carbon dioxide the blood carries is in solution in the plasma, 20% combines with haemoglobin and 75% transports in the form of bicarbonates.
THE HEART

A 4-chamber pump. The upper chambers on each side are called the atria.
The atrium receives blood and then pumps it into the ventricles below. The ventricles then pump blood away from the heart.
The left side of the heart is larger than the right side.
The left side supplies the whole body with blood.
The carotid arteries branch off the aorta immediately and supply blood to the brain.
Oxygen-poor blood returns to the right side of the heart.
Arteries carry blood Away from the heart.
Veins carry blood toward the heart.
Capillaries are microscopic vessels between arteries and veins; gas exchanges occur in the capillaries.
Oxidate metabolism is the process of turning chemical energy into usable energy. This means that oxygen is used and carbon dioxide is released. Oxygen is metabolised (body uses)
The respiratory reflex in the brain monitors the CO2 level. When the Carbon Dioxide rises, the diaphragm is signalled to flex downward. Carbon Dioxide triggers the urge to breathe.
Nitrogen is an inert substance. Nitrogen is not metabolised (Inert- the body does not use it)
Haemoglobin carries Oxygen
The reason we put a distressed diver on 100% oxygen is to increase the partial pressure of oxygen and eliminate excessive levels of nitrogen.
Due to gas density, the deeper you’re diving, the more easily you can over-exert yourself.
CARBON DIOXIDE
HYPERCAPNIA
is TOO MUCH carbon dioxide:
HypEr
(too much)
HypErCApnia
Excessive
CArbon – Dioxide
• Caused by dead air space, skip breathing (holding the breath periodically), shallow rapid breathing, overexertion, or a combination of these. In very rare cases, the air supply may be high in carbon dioxide.
• Causes headache and increased breathing. In severe cases, confusion and loss of consciousness.
• Avoid by breathing deeply and normally, not skip breathing, and avoiding overexertion.
• Because air is denser at depth, it is easier to over-exert yourself
• Hard work, overexertion, and improper breathing may primarily increase the level of carbon dioxide in the body, contributing to gas narcosis on deeper dives
DEAD AIR SPACES

Vital capacity – The maximum volume that can be inhaled after total expiration.
Residual volume – The air left in the lungs after a complete exhalation.
Dead air spaces – The portion of the diver’s tidal volume that plays no direct part in gas exchange.

When you inhale, the first gas drawn into your alveoli is the gas left in your breathing passages from your previous expiration. This gas is higher in CO2 than the fresh gas that you are breathing. Adding a snorkel or regulator increases the amount of dead air you inhale; this means that dead air becomes a larger portion of each breath, thus raising the CO2 in the alveoli correspondingly - Hypercapnia.
If you encounter a strong current and begin to experience confusion and a feeling of air starvation. You should stop, rest, and breathe slowly and deeply.
HYPOCAPNIA and HYPOXIA
HypO
(too little)
HypOCApnia
Omitted (Insufficient) Carbon Dioxide
HypOXia
Omitted (insufficient)
Oxygen
Hypocapnia (also called hypocarbia) is insufficient carbon dioxide, and it can cause physiological problems:
Generally, occurs after excessive voluntary hyperventilation or unintentional hyperventilation due to stress or fright.
Symptoms are light headiness which can be followed by fainting.
Hypocapnia during breath holding may lead directly to shallow-water blackout without warning due to hypoxia.
CARBON MONOXIDE POISONING
CONTAMINATED AIR
Dalton's law: The total pressure of a mixture of gasses is equal to the sum of the partial pressure of each of the different gases in the mixture. Each gas acts alone and is not influenced by the presence of other gases.

Breathing Carbon Monoxide at depth can be dangerous because the symptoms are not noticeable due to the tissues still receiving enough oxygen, despite the carbon monoxide bonding with the haemoglobin, because of high partial pressure (Dalton's Law) meeting tissue demands. Haemoglobin carries less and less oxygen as more Carbon Monoxide bonds with it. Upon surfacing, the plasma can no longer carry enough dissolved oxygen and the diver blacks from hypoxia.
Bonds generally up to 200 X more readily with haemoglobin than oxygen and can take up to 12 hours to eliminate from your body.
Generally, this happens due to contaminated air from various oil-derived hydrocarbons.
Carbon monoxide is a product of combustion. Poisoning generally originates with a compressor system problem that overwhelms the filters, resulting in a contaminated gas supply. Carbon monoxide can enter a diver’s air if the air compressor intake valve is placed too close to the engine exhaust or if the lubricating oil in a malfunctioning compressor becomes hot enough to partially combust, producing carbon monoxide. It can go unnoticed at first because carbon monoxide lacks both odour and taste. For divers, this can be avoided by only filling your tanks at refutable air stations.
Bonds 200 times more with haemoglobin than oxygen
Up to 12 hours to eliminate from the body
Symptoms may include cherry red lips and nail beds, headache, nausea, weakness, clumsiness, confusion, narrow vision, and unconsciousness.
Severe cases of carbon monoxide poisoning can cause seizures, loss of consciousness, or coma. Diagnosis is with a blood test. As time passes, the blood level decreases, so in order to make the diagnosis, the test should be done as soon as possible. The diver’s air supply can also be tested for carbon monoxide.

Treatment: - Fresh air, oxygen if available. Medical attention is needed in all cases.
Severe cases – give the diver pure oxygen and contact emergency medical care. High blood levels of oxygen help eliminate carbon monoxide from the blood but does not always cause organ damage to resolve. For people with severe poisoning, people may be given high-pressure oxygen therapy in a hyperbaric chamber, available at certain medical centres.
Smoking raises carbon monoxide levels in the blood 3 to 12 time’s normal
OXYGEN TOXICITY
There are two types of Oxygen Toxicity.

Pulmonary Toxicity
• Caused by continuous exposure to elevated oxygen partial pressure greater than .05 bar.
• Symptoms and signs include burning in the chest and irritated cough.
Usually resolves itself by ceasing diving for several days. Not considered immediately life-threatening or hazardous.
Central Nervous System (CNS) Toxicity
Oxygen becomes toxic at partial pressures above 1.4 ata. This toxicity can cause convulsions that are dangerous underwater, although individual thresholds vary widely and depend upon environmental conditions and exertion levels.
Caused by exposure to oxygen partial pressures greater than 1.4 BAR
Symptoms and signs include Visual disturbances, Ear ringing, Nausea, Twitching muscles, Irritability, and Dizziness. V.E.N.T.I.D.

The most serious is convulsion (hyperoxic seizure - excessive O2), which can cause the diver to drown. These powerful convulsions may cause unconsciousness, and the diver may lose the regulator mouthpiece.
At the surface, pure oxygen (100%) has a partial pressure of 1.0 atmospheres (ata). As pressure increases by 1atm for every 10 msw, a diver will be at the 1.4 ata threshold at 4 m / 13 ft. This is also called the oxygen window as decompression times can be shortened by breathing pure oxygen at depth 6m or less. This is because, at rest, the threshold at which toxicity occurs is raised (1.6 ata).
When using Enriched Air, remember to stay shallow.
100% pure oxygen can be toxic in just 4 meters of water.
4÷10+1=1.4
PPO2 1.4 x 1 = 1.4ata
Diving with air at 21% and within the limits of recreational diving (up to 40 meters), divers will not reach a 1.4 bar/ata
40÷10+1=5 ata
PPO2 = 5 x .21=1.05ata
Breathing normal air, the percentage is about 21% oxygen, so at the surface, the partial pressure is around 0.21 ata. The threshold of 1.4 atm would be reached at around 56 m.
56÷10+1=6.6ata
PPO2=6.6 x .21 = 1.386ata (rounded to approx 1.4ata)
GAS (NITROGEN) NARCOSIS
Gas narcosis- also known as nitrogen narcosis, inert gas narcosis, raptures of the deep (coined by Jacques Cousteau in his book "The Silent World") and the Martini effect (comparing it to drinking one martini for every 10 mt after 30mt), is caused by the anesthetic effect of certain gases at high pressure.

Nitrogen Narcosis is caused by breathing high partial pressures of Nitrogen.
Using either air OR enriched air, Nitrogen becomes narcotic around 30mts.
Nitrogen is an inert gas which means that the body does not metabolise it (what goes in must come out).
Most gases can cause anaesthesia under high pressure. Helium has no known narcotic effect under very high pressure, which is why it is used by technical and commercial divers.
Not directly hazardous. Hazards come from impaired judgement and coordination, a false sense of security, euphoria and a lack of concern for safety that may lead to bad decisions. Divers may also feel anxious or uncomfortable.
Narcosis may be alleviated by simply bringing the diver to shallower depths, with no after-effects.
Nitrogen narcosis is an effect similar to alcohol intoxication or nitrous oxide inhalation. It can occur in shallow dives but traditionally can start to become a problem in the 20 - 30 msw (meters sea water) range, equivalent to 2.37 - 3.16 bar of absolute breathing air, and is caused by the partial pressure of nitrogen in the blood.
Nitrogen levels become narcotic when it reaches +/- 3 Bar.
3 Bar ÷ 0.79 (If using air
= 3.7 Bar = 27m (Ambient)
All gases that can be breathed, with the exception of helium and possibly neon, have a narcotic effect, although the exact reason for this phenomenon is not clearly understood.
What we do know is that as the depth increases, mental impairment becomes a hazard.
How severe the effect depends upon the environment and susceptibility of the individual, but it generally is accompanied by a feeling of euphoria and well-being that can lead to impaired judgement and confusion and can put a diver at risk.
Narcosis is a reversible alteration in conscience that can be resolved in a few minutes by simply ascending to a shallower depth, with no long-term effects. Theoretically, it affects all divers past 30mt (although it can happen shallower), and as such, it rarely develops into a serious problem in recreational diving if divers are aware of its symptoms and are able to ascend to manage it.
As there is no way to avoid it, being aware of the symptoms is important to avoid making simple errors that can put you in dangerous situations, like not managing the air supply.

Building up dive depths at the start of the season and not diving a deep dive directly after a long time out of the water can help reduce the effect.
The limit of recreational diving is generally 40 m (130 ft). When diving greater than these depths, narcosis and oxygen toxicity become critical risk factors, and special training is required for the use of different gas blends to accommodate this. The use of helium-containing gas mixtures such as trimix or heliox prevents narcosis by replacing some or all of the inert gas (gases that the body does not metabolise) with non-narcotic helium.
Hard work, overexertion and improper breathing may primarily increase the level of carbon dioxide in the body, contributing to gas narcosis on deeper dives.
GAS MIXTURES
Nitrox
Nitrox is a mixture of nitrogen and oxygen but with less nitrogen and more oxygen than found in normal air. Nitrox can be used at moderate depths (generally less than the maximum limits of recreational diving) without risking oxygen toxicity and greatly reduced decompression time.
Trimix
Trimix is a mixture of helium, oxygen and a third gas, usually nitrogen. Trimix has the advantage of reducing nitrogen and oxygen concentrations so that the divers may descend to greater depths without the problems of oxygen toxicity or nitrogen narcosis. The density of the breathing mixture is also reduced, which makes it easier to breathe at higher pressures.
Closed Circuit rebreather
Closed-circuit rebreather systems recapture oxygen in exhaled breathing gas, allowing a diver to carry much less breathing gas. In addition, modern closed-circuit rebreathers constantly monitor oxygen levels in the breathing mixture and are able to adjust the oxygen concentration to a level that is optimum for the divers’ depth. The result is much shorter decompression times and much less risk of oxygen toxicity.

NITROGEN ABSORPTION AND ELIMINATION
HENRY’S LAW: if the pressure increases (Gets More/Greater), the more gas will be dissolved (Go into) the liquid. If the pressure is decreased (Gets less), the gas will come out of the liquid.
Our bodies use the Oxygen from our lungs when we breathe and transport it throughout our body. Oxidative metabolism is how our cells use oxygen to convert chemical energy into usable energy.
Our bodies are mostly liquid, and Nitrogen is an inert gas, which means that the body cannot use it, so while diving, nitrogen dissolves into and out of body tissues until reaching the surrounding pressure (saturation), exposing the body to a higher absorption rate upon descent.
Different parts of the body absorb and release Nitrogen at different rates (half-times), although most recreational dives are too short to reach saturation.
Upon ascent, the nitrogen begins to dissolve out of your tissues, and your body begins to eliminate it, which is where potential decompression sickness problems arise.
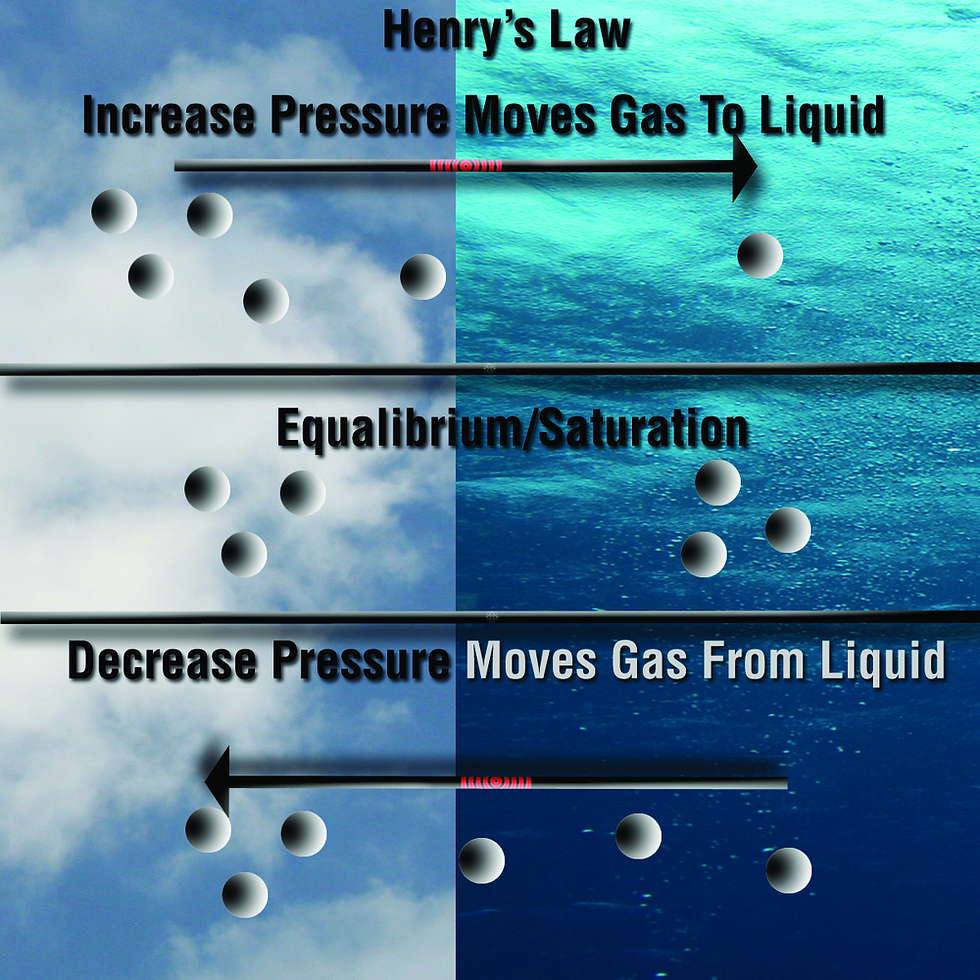
Gas ALWAYS goes from a high pressure to a low pressure, so while ascending, the pressure reduces, and the Nitrogen in the tissues is higher than the pressure of Nitrogen in the air breathed by the diver (Supersaturation). The nitrogen dissolves out of the body tissues, into the air being breathed and is exhaled.
The difference between the pressure of the Nitrogen dissolved in the body and the surrounding (ambient) pressure is called the Pressure Gradient.
At a slow ascent rate, the Nitrogen is released harmlessly and is breathed out.

With a fast ascent rate and the pressure gradient too great, Nitrogen comes out of the solution faster than it can be eliminated and bubbles form. This is Decompression Sickness.
Getting cold reduces blood flow to the extremities (vasoconstriction), thus slowing the elimination of nitrogen.
Technical diving – decompression stops (avoid excessive gas pressure gradient)
Recreational – No-stop diving (doesn't exceed excessive nitrogen in the tissues, so a direct ascent to the surface is possible)
If you would like to test your knowledge on
The Body System and the Effects of Gases
Do the exam below
THE PHYSIOLOGICAL EFFECTS OF APNEA
APNEA

During APNEA (breath holding), the circulatory system uses oxygen stored in the lungs.
You can increase breath-hold time by first hyperventilating (breathing deeply and rapidly) three or four times. Doing so reduces circulatory carbon dioxide, so it takes longer to get enough CO2 to trigger the need to breathe. Too much hyperventilation may lead to shallow water blackout and is no longer allowed during apnea dives.
HypErventilation
Excessive Ventilation
Diaphragm breathing is used before breath-hold dives rather than hyperventilation.
When you breathe diaphragmatically, your abdomen expands outward as your lungs fill with air. Diaphragmatic breathing is an efficient way to breathe and is not only used by freedivers, but by athletes, singers, and other performers to improve their breathing too. Diaphragmatic breathing practice is perfect for high-stress situations, including in the workplace.
SHALLOW WATER BLACKOUT
Dalton's law: The total pressure of a mixture of gasses is equal to the sum of the partial pressure of each of the different gases in the mixture. Each gas acts alone and is not influenced by the presence of other gases.
Caused by excessive hyperventilation, depleting a diver’s carbon dioxide level causing hypocapnia
Shallow-water blackout gets its name because it occurs on an ascent near the surface. Due to a low carbon dioxide level, there is no stimulus to breathe. The diver stays underwater longer, using more oxygen. The divers body depletes the oxygen supply but increased partial pressure of oxygen at depth in the alveoli allows haemoglobin to continue using oxygen even after dropping below a level that would cause unconsciousness at the surface. When the diver ascends, the oxygen partial pressure in the lungs falls rapidly, so the haemoglobin can no longer bond with oxygen and supply the body. Consequently, hypoxia results instantly, and the diver blacks out.
Shallow water blackout can also occur if the diver stays too long under the water and depletes their oxygen.
TACHYCARDIA AND BRADYCARDIA

Tachycardia is the speeding up of the heart rate.
Bradycardia is the slowing of the heart rate.
When you first take a deep breath, tachycardia occurs, followed by bradycardia when you breathe out.
The bradycardia response to apnea has sometimes been called the mammalian diving reflex/mammalian reflex. This reflex is associated with cold water on the face, although it does not appear to reduce O2 consumption in humans as it does in marine mammals, only slowing the heart.
The mammalian diving reflex refers to the tendency for a breath-hold diver’s heart rate to decrease when submerged in cold water.
If you would like to test your knowledge on
The Physiological Effects of Apnea
Do the exam below
DECOMPRESSION SICKNESS AND LUNG OVER-EXPANSION INJURIES
DECOMPRESSION SICKNESS
HENRY’S LAW: if the pressure increases (Gets More/Greater), the more gas will be dissolved (Go into) the liquid. If the pressure is decreased (Gets less), the gas will come out of the liquid.

There are two types of decompression sickness/ DCS:
- Type I: ‘Pain only’, Not immediately life-threatening - Type II: May be immediately life-threatening involving the central nervous system
Decompression Sickness is caused by Nitrogen bubbles that form in the tissues and bloodstream and block Oxygen to the tissues.
Upon ascent, the nitrogen begins to dissolve out of your tissues, and your body begins to eliminate it, which is where potential decompression sickness problems arise.
Bubbles exist after every dive. If these bubbles are too few and small (silent bubbles), they have no effect. However, if there are enough bubbles, the volume can cause Decompression Sickness.
TYPE I | TYPE II |
Bubbles coming out of solution in skin capillaries, characterised by a red rash in patches, usually on the shoulders and upper chest. Not serious by itself but may be an indication of further decompression problems and the possibility of more serious symptoms 2. Joint and limb pain decompression Sickness Joint or limb pain occurs in about 76% of DCS. Pain symptoms may be located in more than one place on the same limb, e.g., the shoulder and elbow. Bi-symmetrical symptoms are unusual. Considered serious | 1. Neurological decompression sickness
Can affect movement, touch, and life support functions such as breathing and heartbeat. Symptoms, therefore, include peripheral tingling and numbness, unconsciousness, respiratory arrest, and paralysis. It usually affects the spinal cord, thus causing numbness and paralysis in the lower extremities. May become paralysed from the neck down. Considered most serious.
2. Pulmonary decompression sickness
DCS manifesting itself in lung capillaries signals the possible onset of life-threatening symptoms. It’s rare. Silent bubbles and microbubbles reaching the pulmonary capillaries normally diffuse into the alveoli or, in rare cases, may travel into the arterial system and cause neurological DCS. The heart rate will rise, and blood pressure will drop. Without treatment, the circulatory system may fail completely. Pulmonary decompression sickness creates breathing pain and a short irritating cough. The victim feels air-starved, hence the nickname ‘the chokes. Symptoms progress rapidly and may lead to shock.
3. Cerebral decompression sickness
Results from bubbles passing through the pulmonary capillaries and travelling to the brain via the carotid arteries. Symptoms include blurred vision, headache, confusion, unconsciousness, and death.
|
Signs and Symptoms of DCS Type I | Signs and Symptoms of DCS Type II |
joint pain fatigue malaise paresthesia muscle aches skin problems such as rashes or itches | Headaches Seizures Behavioural changes Visual disturbances Numbness Paralysis Fatigue Unconsciousness Coma Death |
Signs and Symptoms of Decompression Sickness
Unusual fatigue
Skin itch
Pain in joints or arm, leg or torso muscles
Dizziness or vertigo
Ringing in the ears
Numbness, tingling and/or paralysis
Shortness of breath
A blotchy rash
Muscle weakness or paralysis
Difficulty urinating
Confusion, personality changes or bizarre behaviour
Amnesia
Tremors
Staggering
Coughing up bloody, frothy sputum
Unconsciousness or collapse
FACTORS PREDISPOSING DCS
Individual variations in physiology & any actions taken
Body Fat Nitrogen is more soluble in fat than in water, so a diver who has excessive body fat may absorb more nitrogen during a dive than the decompression models predict
Exercise Before & After While intense exercise 12 hours before a dive might have a protective effect, immediately before a dive predisposes a diver to DCS as the absorption and elimination of nitrogen are affected. Exercise immediately after may increase blood pressure and can encourage bubble movement
Age As a person ages, the circulatory and respiratory systems work less efficiently, affecting gas exchange. As we age, our bodies tend to have higher body fat
Dehydration Reduces the amount of blood available for the gas exchange affecting gas elimination
Injury & Illness May potentially affect gas elimination. Recently healed injuries may produce local circulation issues, and injuries can produce a general reduction in circulation efficiency
Alcohol Before and After Before a dive, even small amounts of alcohol can accelerate circulation, which can result in tissue loading with inert gasses. It also contributes to gas narcosis. After a dive, alcohol dilates capillaries, increasing nitrogen release and contributing to bubble formation
Carbon Dioxide Hypercapnia can interfere with the circulatory system affecting gas exchange by dilating capillaries and increasing or altering inert gas (nitrogen) uptake
Cold Before and After If a diver is cold throughout the dive, then the circulatory patterns change little. If a diver starts warm and finishes cold, then the diver will have normal circulation on the uptake of inert gases but restricted circulation during the elimination of the inert gases. After a dive, if the diver is cold, they may not have adequate peripheral circulation.
Hot showers after a dive If the diver is cold then has a hot shower then the likelihood of bubbles forming in their tissues increases. Exposure to heat reduces tissues' capacity to hold inert gas in solution.
Altitude & Flying After Diving Reduced atmospheric pressure at altitude increases the pressure gradient between the gases dissolved in your tissues and the ambient pressure.
Patent Forman Ovale (PFO) Hole in the heart Normally, harmless bubbles in the venous side of the heart on the way to the lungs to be eliminated may pass to the arterial side of the heart, and this may cause more severe forms of DCS.
History of DCS An initial incident of DCS may injure or degrade the body system, making a diver more predisposed to DCS.
Smoking circulation in small blood vessels is reduced by 19 per cent after just two cigarettes. Poor gas exchange and increased risk of decompression sickness results.
Most of these predisposing factors somehow result in, or cause a change in circulation.
LUNG OVER-EXPANSION INJURY
Breath held ascents
Diving with a chest cold
Local blockage in the lungs due to loss of surfactant (due to smoking)
BOYLES LAW: If temperature remains constant both volume and density of a gas are affected in proportion to the atmospheric pressure and inversely to each other.
Lung over-expansion injuries have the same first aid as DCS
First aid is the same, irrelevant of the type of lung over-expansion injury
Giving oxygen helps supply tissues deprived of blood flow by bubbles.
A diver suspected of having a lung expansion injury should be treated as if it’s an air embolism because this is the most serious lung injury.
Treatment of air embolism requires recompression to reduce bubble size (as in DCS).
Subcutaneous Emphysema

Caused by an air rupture gathers in the base of the neck, around the collar bone. The victim may feel fullness in the neck, the voice may change, and skin will crackle to the touch.
Mediastinal Emphysema

Gas gathers in the mediastinal (centre of the chest). It is far less serious than either air embolism or pneumothorax. The accumulating air presses on the heart and major blood vessels, interfering with circulation. A victim may feel faint and short of breath due to this impaired circulation.
Pneumothorax

Caused by a rupture between the lungs and the chest wall, causing the lungs to collapse. May cause chest pain, and the victim may cough up blood.
Arterial Gas Embolism (AGE)

Air enters the bloodstream and flows into the arteries. Immediately life-threatening, and bubbles can lodge anywhere. The most common is to flow through Carotid Arteries and cause Cerebral Air Embolism. Signs and symptoms like stroke, dizziness, confusion, shock, paralysis, personality change, unconsciousness and death.
Signs and Symptoms of Lung Over-Expansion Injuries
Paralysis, particularly on one side of the body
Unconsciousness
Dizziness and confusion
Coughing up blood
Loss of vision
Change in voice
Heavy chest pain and difficulty breathing
FACTORS PREDISPOSING LUNG OVEREXPANSION INJURY
Individual variations in physiology & any actions taken
Breath held Ascent
Smoking increases mucus within your air passages. Whenever you exhale, some of your lung bronchioles and alveoli collapse, creating a momentary internal airflow blockage. Abstain at least 10 to 12 hours before and after diving.
Chest congestion Smoking and lung congestion can pose risks of gas trapping and lung overexpansion injuries. Don’t dive with any form of chest congestion.
Smoking and chest congestion can contribute to lung overexpansion in the ascent during a breath-hold dive.
DECOMPRESSION ILLNESS
DECOMPRESSION SICKNESS
= NITROGEN IN THE BODY COMING OUT TOO FAST
DECOMPRESSION ILLNESS
= DECOMPRESSION SICKNESS + LUNG OVER EXPANSION INJURIES
Signs and symptoms of DCS and lung overexpansion injuries are quite often the same
1ST Aid is the same for both DCS and Lung Overexpansion Injury, hence a blanket term of DECOMPRESSION ILLNESS is used for both.
1. Treat all DCI as serious, even pain-only DCS.
2. Give the patient oxygen (preferably 100 per cent).
a. Lowers alveolar nitrogen to accelerate elimination from tissues
b. Raises blood oxygen levels to assist tissues with blood flow reduced by bubble blockage.
3. Keep a breathing patient lying level on the left side, head supported (recovery position).
a. Helps keep the airway clear if the patient vomits.
b. Lying level helps ensure blood flow to the brain.
c. Advise patient not to sit up or walk around, even during transport or if feeling better.
4. Lay the non-breathing patient on the back for rescue breathing/CPR.
5. Contact emergency medical care.
If necessary for treatment, a physician familiar with hyperbaric medicine can determine the specific mechanism of injury later after the diver is in emergency medical care.
Never enter the water for re-compression.
DCI treatment requires putting the patient in a recompression chamber.
Treatment involves a long slow decompression with oxygen and drug therapy.
The sooner therapy begins, the greater the chance of recovery without permanent injury.
Upon surfacing, Decompression Sickness occurs within a few hours and up to 36 hours.
Lung Overexpansion occurs within a few minutes.
SILENT BUBBLES

The introduction of the Doppler Ultrasound Detector in the 1970s discovered small bubbles in the bloodstream.
These bubbles travel to the lungs, where the pulmonary capillaries trap them. The gas in these bubbles then diffuses harmlessly into your alveoli. (Except in rare cases where they accumulate faster than they diffuse, as there as so many of them)
Silent bubbles are found after some dives, especially those close to table/ computer limits.
They are called Silent Bubbles because they do not produce DCS.
If you would like to test your knowledge on
Decompression Sickness and Lung Over Expansion Injuries
Do the exam below
PRESSURE-RELATED INJURIES AND THE CAROTID SINUS REFLEX
BAROTRAUMAS
A pressure-related injury.
A barotrauma of descent is called a squeeze or block, and a barotrauma of an ascent is called a reverse squeeze or reverse block.
THE EAR

3 PARTS
OUTER
MIDDLE
INNER
The outer ear is made up of the pinna and the ear canal. It is open to water and air pressure. This collects sounds and directs them into the ear canal toward the ear drum (tympanic membrane).
The middle ear - The eardrum is the start of the middle ear and seals it from water and air pressure. The eardrum is connected to three bones called the ossicles, and these conduct and magnify vibrations. This part of the ear is most affected by changes in pressure.
The inner ear - Vibrations go from the ossicles into the cochlea, an inner ear organ filled with a liquid called perilymph. The ossicles attach to the oval window of the cochlea that flexes in and out in response to ossicle vibration. As the oval window flexes, it pushes against the perilymph causing pressure wave to oscillate through the cochlea. The pressure waves stimulate auditory nerve endings in the cochlea, turning the pressure waves into nerve impulses the brain understands. The round window on the cochlea acts as a pressure compensator, flexing outward when the oval window flexes inward against the incompressible perilymph and flexing inward when the oval window flexes outward. Without this action, the hearing would not take place.
The Vestibular Canal controls balance as well as orientation. They do not contribute to hearing but are connected to the cochlea. Pressure changes result in responses to balance as well as hearing.
The Eustachian Tube connects the middle ear, which is dry and air-filled and the main pressure concern, to the throat, which allows gas to flow through it. The outer ear is open to the environment and, therefore, always in equilibrium with the surrounding pressure. The inner ear is liquid-filled and, therefore, unaffected by pressure. This area is responsible for our balance.
Descending: Pressure pushes on the eardrum, diver feels discomfort.
Equalizing: The diver forces air up the Eustachian tube to equalize the middle ear and alleviate discomfort.
Ascending: Air normally exits the Eustachian tube easily and seldom needs to assist in the regulation of pressure.
Ossicles connect to the cochlea at the oval window, which flexes in and out with vibrations.
The round window on the cochlea flexes out when the oval window flexes in to compensate.
Equalisation - controlled by the Valsalva or the Frenze manoeuvre
Valsalva uses the diaphragm and attempts to exhale against a pinched nose. This method is mainly used when starting diving.
Frenze Manoeuvre uses throat muscles to compress air against a pinched nose. This method minimises round-window rupture.
SQUEEZE:
involves the hydrostatic pressure forcing body tissues into uncompensated air spaces. So, we can say that the pressure on the outside is greater than the pressure on the inside. It is the phenomenon of a shrinking air space as the pressure rises and the volume reduces during descent, causing pain to the diver.
Middle Ear Squeeze is where the diver descends and is unable to equalize. The hydrostatic pressure forces the eardrum inwards towards the unequalised airspace. The pressure forces fluids and blood from tissue surrounding the middle ear's air space. The diver's ear feels “full”, and the sharp pain diminishes.
Eardrum Rupture occurs if a diver descends faster than the hydrostatic pressure can compensate with liquids, causing the eardrum to rupture. The diver feels a sharp pain followed by instant relief as the rupture allows the water into the middle ear, equalising the pressure. The cooler water can cause vertigo and disorientation as it cools the vestibular canals. Usually heals without complication but requires medical attention to prevent infection and permanent damage that may be caused by contaminates in the water.
Earplug problems. Ear plugs create air spaces in the canal between the plug and the ear drum that cannot be equalized. If the diver tries to equalise, this will make the problem worse because adding air to the middle ear increases the pressure difference. In addition, hydrostatic pressure may force the plug deeper into the ear.
Reverse Squeeze. Ears equalize on the descent, but congestion at depth prevents air from escaping through the Eustachian tube upon ascent. The eardrum flexes outward. This happens when divers use decongestants that wear off during the dive. Like a middle ear squeeze, except the eardrum flexes outwards. Sometimes reverse equalisation can help. This is the worst situation of a squeeze for a diver near the end of a dive.
Round Window Rupture: This is the most serious ear injury. If equalisation is delayed, the round window in the ear bulges outwards in response to the pressure transmitted to the cochlea. If the diver at the same time equalises using a forceful or lengthy Valsalva, the perilymph pressure increases, combines with the pressure transmitted from the eardrum and can rupture the round window. This rupture causes the diver’s ears to feel blocked, and the diver may have a hearing reduction, often with ringing sounds and vertigo. This is a serious injury, and failure to have it treated can lead to a permanent hearing reduction.
Swimmers Ear (Otitis externa) Not a barotrauma but very common. Results from the pH of the ear canal becoming alkaline instead of acidic due to repeated exposure to water and humidity. Symptoms range from an itch, closure of the external ear canal, swelling, fever, and pain. Treat the ear before the symptoms appear with an over-the-counter alcohol mix by flushing the ear canal. Any wax should be removed periodically.
Sinus Squeeze. A diver may or may not feel pain upon descending with blocked sinuses as the pressure pushes in on the trapped air. A rapid descent may cause pain in the eyes, teeth, or cheekbones. As hydrostatic pressure forces blood and fluid from the surrounding tissue into the air pockets, any pain is usually alleviated.
Upon ascent, the air re-expands, the blood and fluids are pushed into the nasal cavity, and the diver surfaces with blood in the mask. While it looks quite dramatic, it will heal on its own and requires little or no medical attention unless accompanied by severe pain.
Mask Squeeze. Upon descent, the diver normally naturally equalizes the mask by exhaling through the nose. Failure to do so can create unequal pressure between the mask and the face. This can result in various degrees of facial barotrauma or injury to the soft tissues of your face contained within the mask. Imagine your face in a suction cup. The soft tissues beneath the mask, especially around the eye, swell and discolour (such as redness or bruising). While it looks traumatic, it is a bruise, and your body will eventually reabsorb the effect of your mask squeeze. Your physician or an eye specialist should address eye pain or visual disturbances such as blurred vision or loss of part of the visual field immediately, although this is extremely rare from a mask squeeze.
Dry suit squeeze occurs during a rapid descent if you don’t equalize the air spaces. The air pocket inside your dry suit is squeezed, and as a result, the material of your dry suit is pressed against your body. Most commonly occurs when a rapid descent when the dry suit inflator is accidentally left disconnected. Dry suit squeeze is particularly uncomfortable around the valves and seams of your suit. A tight neck seal on a newly replaced dry suit seal may cause a diver to feel light-headed. Seals can be trimmed with scissors until the correct fit is obtained.
Lung Squeeze (Thoracic squeeze) can happen if a person dives to a depth that compresses the lungs below their residual volume (the lowest volume they reach naturally). Although this would mean a free dive deeper than 30m or exhaling and descending with empty lungs. This could compress the lungs below residual volume in only 2-3m of water. If compression continues, the delicate lung tissue may rupture and allow tissue fluids to enter the lung spaces and tubules. The outer linings of the lungs (pleural sacs) may separate from the chest wall, and the lung may collapse. The predominant symptom would be pain when the pressure becomes too great, and this is relieved by ascending. If the squeeze has been enough to cause lung damage, the diver will have trouble breathing, may exhale frothy blood, and may even become unconscious. Artificial respiration may be necessary if the breathing has stopped. Any symptoms of thoracic squeeze call for prompt medical attention.
CAROTID SINUS REFLEX

Carotid Sinus receptors monitor the pressure of arterial blood reaching the brain through the carotid arteries.
Low blood pressure triggers a higher heart rate, and high blood pressure triggers a lower heart rate.
Receptors interpret pressure from an excessively tight hood or wet suit constricting the neck as high blood pressure.
The heart rate slows, reducing the flow to the brain but the pressure remains, causing a yet slower heart rate.
The diver feels uncomfortable and lightheaded but may lose consciousness if constriction continues unrelieved.
Carotid Sinus reflex reduces fresh blood flow to the brain, raises blood pressure in the head and slows the heart rate.
If you would like to test your knowledge on
Pressure Related Injuries and the Carotid Sinus Reflex
Do the exam below
THERMAL EFFECTS ON THE BODY AND DIVER STRESS
EXCESSIVE HEAT – HYPERTHERMIA
As the body heats up:- - Initially, skin capillaries dilate, allowing heat from the blood to radiate. - Perspiration follows, cooling the skin. - The pulse accelerates to circulate blood more rapidly. - Breathing increases.
Heat exhaustion does not usually need emergency medical help if you can cool down within 30 minutes. If it turns into a heatstroke, it needs to be treated as an emergency. Heat stroke can cause permanent disability or death if the person does not receive emergency treatment.

HEAT EXHAUSTION
Strenuous activity in the sun, accompanied by wearing a heavy exposure suit, can lead to heat exhaustion when the body works at a maximum capacity to keep your core temperature from rising.
Symptoms of heat exhaustion include:
Tiredness and weakness
Feeling faint or dizzy
A headache
Muscle cramps
Feeling and being sick
Pale, cold, clammy skin
Heavy sweating
Intense thirst
Weak rapid breathing
A weak rapid pulse (faster than 100 per minute)
Urinating less often and having much darker urine than usual (indicating dehydration)
If someone has heat exhaustion, follow these 4 steps
Move them to a cool place.
Remove all unnecessary clothing like a jacket or socks.
Get them to drink a sports or rehydration drink or cool water.
Cool their skin – spray or sponge them with cool water and fan them. Cold packs, wrapped in a cloth and put under the armpits or on the neck, are good, too.
Stay with them until they're better.
They should start to cool down and feel better within 30 minutes.
HEAT STROKE
If a diver with heat exhaustion remains hot or continues to heat, the physiological control mechanism will eventually fail and result in heat stroke.
Symptoms of heat stroke include:
Confusion, altered mental status, slurred speech
Headache
Strong rapid pulse
Loss of consciousness (coma)
Hot, dry skin to touch
Seizures
Very high body temperature
Fatal if treatment delayed
If someone has a heat stroke
Call emergency services immediately and put the person in a recovery position while you are waiting for help.
Stay with the person until emergency medical services arrive.
Move the person to a shaded, cool area and remove outer clothing.
Cool the person quickly using the following methods:
With a cold water or ice bath, if possible
Wet the skin
Place cold, wet cloths on the skin
Soak clothing with cool water
Circulate the air around the worker to speed cooling.
Place cold, wet cloths or ice on the head, neck, armpits, and groin, or soak the clothing with cool water.
Do not drink fluids while waiting for emergency services, as fluids may enter the lungs through the trachea or airway.
EXCESSIVE COLD – HYPOTHERMIA
(Insufficient heat)
As the body cools down: -
- Temperature centres in the hands, feet and head trigger heat-conserving responses that start with a change in circulation. - Blood flow to the extremities slows through vasoconstriction (constriction of blood vessels) to reduce heat loss.
- This results in numbness in the fingers and toes after a long exposure.
- Then, the body reacts by shivering, which generates heat through muscle activity and accelerated metabolism. - The head loses considerable heat because the body can’t reduce blood supply to the brain


Mild hypothermia
It starts with uncontrollable shivering and impaired coordination, numbness in fingers and toes, along with a reduction in core temperature, which lowers to 34 C°/ 93 F°.
For a diver with mild hypothermia, remove any wet clothing, wrap in insulating clothing/blanket, and drink a warm, non-alcoholic drink.
Advanced Hypothermia
As the condition worsens, shivering and vasoconstriction cease. The diver suddenly feels comfortable as warm blood rushes to the skin. This is dangerous because the body now loses heat at an uncontrolled rate, and the core temperature drops rapidly. The diver then becomes drowsy, uncoordinated, and forgetful. If unchecked, the diver loses consciousness, followed by coma and death.
First-aid tips
Be gentle. When assisting a person experiencing hypothermia, handle them with care, limit movements to only what is necessary, and avoid massaging or rubbing them as excessive and jarring movements could result in cardiac arrest.
Move the person out of the cold. If someone is suffering from the cold, try to move them to a warm and dry location. If it's not possible to move them, protect them from the cold and wind as much as you can. It's best to keep them lying down if that's possible.
Remove wet clothing. If a person is wearing wet clothes, remove them carefully. Cut away the clothes only if necessary to avoid causing further harm.
Cover the person with blankets. Layer dry blankets or coats to warm the person, covering their head and leaving only the face exposed.
Insulate the person's body from the cold ground. If the person is outside, lay them on their back on a warm surface such as a blanket.
Monitor breathing. A person with severe hypothermia may be unresponsive and without a detectable pulse or breathing. If breathing is absent or appears dangerously low or shallow, begin CPR immediately if you are trained.
Provide warm beverages. If the person is conscious and able to swallow, offer a warm, non-alcoholic and non-caffeinated beverage to help raise the body temperature.
Use warm, dry compresses. To provide first-aid for someone, you can use a warm compress. You can either use a plastic fluid-filled bag that warms up when squeezed, or you can make a makeshift compress by filling a plastic bottle with warm water or using a dryer-warmed towel. However, it is recommended to apply the compress only to the neck, chest wall or groin.
Don't apply a warm compress to the arms or legs. Applying heat to the arms and legs can cause cold blood to flow back towards the heart, lungs, and brain, leading to a drop in core body temperature, which can be fatal.
Don't apply direct heat. Do not use hot water, heating pads, or lamps to warm someone up, as it can damage the skin and potentially cause severe heart problems.
Medical treatment
Emergency medical care for hypothermia may include interventions to raise body temperature, depending on its severity.
Passive rewarming. For someone experiencing mild hypothermia, covering them with heated blankets and offering warm fluids to drink is sufficient.
Blood rewarming. One way to warm blood that has been drawn is to recirculate it back into the body. This can be done through a hemodialysis machine, which is typically used to filter blood in individuals with kidney problems. In some cases, heart bypass machines may also be used to warm blood.
Warm intravenous fluids. A solution of warm saline can be infused into a vein to help raise the body temperature.
Airway rewarming. The use of a mask or nasal tube to administer humidified oxygen can warm the airways and help raise body temperature.
Irrigation. A warm saltwater solution may be used to warm certain areas of the body, such as the area around the lungs (pleura) or the abdominal cavity (peritoneal cavity). The warm liquid is introduced into the affected area with catheters.
Water has one of the highest heat capacities of all naturally occurring substances. Your body loses heat rapidly when immersed in water.
NEAR DROWNING
A drowning victim is someone who suffocates underwater and cannot be revived. A near-drowning incident is a person who has been revived following asphyxiation underwater. Near drowning victims may display these typical signs and symptoms;
Coughing
Shortness of breath
Rapid breathing
Cyanosis of the lips (blueness)
Convulsions
Unconsciousness
Vomiting
Cessation of breathing or cardiac arrest
Drowning in very cold water can make revival possible, even after fairly long periods of time.
Regardless of how long a person has been submerged, in cases of drowning, the primary first aid for a nonbreathing diver after reaching the surface is immediate rescue breathing.
If a diver loses consciousness during a dive but is fine after, still are at risk. They may appear fully recovered, only to suffer hypoxemia hours after the incident. This is called secondary drowning. Without therapy, this is often fatal.
The terms hypoxia and hypoxemia are not synonymous.
Hypoxemia - a decrease in the partial pressure of oxygen in the blood vessels
Hypoxia - a reduced level of tissue oxygenation
PSYCHOLOGICAL AND PHYSICAL STRESS
Physical Stress
Physical stressors are those that affect the body, causing discomfort, loss of strength and other effects. Even minor annoyances can cause stress and, if left uncorrected, lead to more serious problems.
Common physical stress causes include:
cold and heat
seasickness
gas narcosis
fatigue
illness or injury
alcohol or drugs
discomfort or impaired function caused by ill-fitted or malfunctioning equipment
Psychological stress is stress due to the diver’s reaction to perceived “threats” in the environment, including perceived causes of actual bodily harm and “threats” to self-esteem. The diver’s beliefs and attitudes play a major role in psychological stress, so the stressor may be imagined or real.
Psychological stress often results from physical stress. For example, fatigue or being tired can trigger psychological stress if the diver fears being unable to make it safely to the boat or shore. An overexerting diver can feel air starved and fear that the regulator can’t deliver enough air.
If you would like to test your knowledge on
Thermal Effects on the Body and Diver Stress
Do the exam below
Here you will find all the exams in one place.

If you would like to test your knowledge on
The Body System and the Effects of Gases

If you would like to test your knowledge on
The Physiological Effects of Apnea

If you would like to test your knowledge on
Decompression Sickness and Lung Over Expansion Injuries

If you would like to test your knowledge on
Pressure Related Injuries and the Carotid Sinus Reflex

If you would like to test your knowledge on
Thermal Effects on the Body and Diver Stress



Comments